
Breastfeeding
Infant Feeding in the UK
Creating the right environment to promote and support breastfeeding’ is one of the important health interventions cited by Public Health England2 for enabling the best start for all infants, alongside other initiatives including the protection of perinatal mental health, smoking cessation support during pregnancy, routine neonatal and developmental screening, vaccination, healthy diet and physical activity. The UK Department of Health3, NHS4 and The World Health Organisation (WHO)5 public health recommendation is for babies to be exclusively breastfed for the first 6 months, followed by the introduction complementary solid foods alongside continued breastfeeding, with the WHO specifying ‘up to 2 years of age or beyond’3-5.
The importance of this Public Health recommendation for UK infants has recently be underlined by the Lancet series on Breastfeeding in which 28 systematic reviews and meta-analyses were analysed, including studies from both low/middle and high income countries6.
The authors concluded that:
Our systematic reviews emphasise how important breastfeeding is for all women and children, irrespective of where they live and of whether they are rich or poor. Appropriate breastfeeding practices prevent child morbidity due to diarrhoea, respiratory infections and otitis media. Where infectious diseases are common causes of death, breastfeeding provides major protection, but even in high income populations it lowers mortality from causes such as necrotising enterocolitis and sudden infant death syndrome. Available evidence shows that breastfeeding enhances human capital by increasing intelligence. It also helps nursing women by preventing breast cancer. Additionally, our review suggests likely effects on overweight and diabetes in breastfed children, and on ovarian cancer and diabetes in mothers.
Victora C.G. et al (2016) Lancet Breastfeeding Series
Our understanding of infant feeding trends in the UK has been informed by the national Infant Feeding Survey, conducted every five years between 1975 and 2010. Data collection provided statistics on the initiation and prevalence of breastfeeding and other feeding practices in the first 8-10 months of a baby’s life. Over the lifetime of the survey breastfeeding rates in the UK were seen to rise7. The Survey was decommissioned following 2010 and infant feeding statistics are now calculated from local provider data.
- In England 74% of babies were recorded as receiving breast milk for their first feed in 2017/18 (validated data from NHS Maternity service providers)8.
- The aggregate breastfeeding rate at 6-8 weeks after birth (any breastfeeding) for England for 2017/18 was 42.7% (data voluntarily submitted to Public Health England by Local Authorities)9.
This data suggests lower breastfeeding rates in England compared to those recorded in the final national Infant Feeding survey of 2010 (data correct as of August 2019), although the methods of data collection now used differ considerably. However, the detailed information previously gleaned from the 2010 Infant Feeding Survey can still highlight important issues for the clinician responsible for the health of infants and mothers, regardless of the method of feeding. The 2010 survey also includes important insights into the introduction of complementary solid foods and the safe preparation of formula feeds.
Breastfeeding in the UK
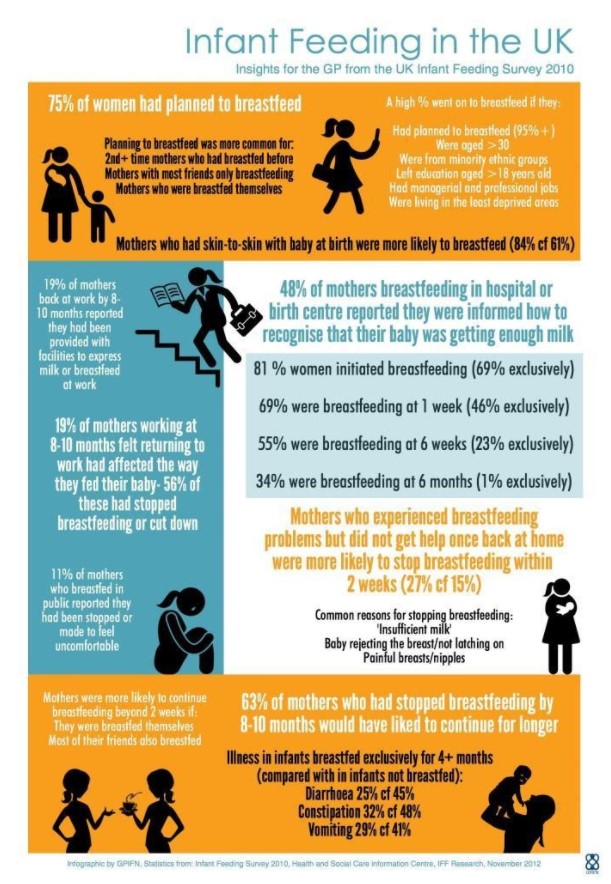
Breastfeeding initiation is known to be higher for babies who experience early skin-to-skin contact and among mothers from certain demographics7 (see infographic below). While breastfeeding initiation remains relatively high in the UK, in 2010 only 1% of mothers maintained exclusive breastfeeding to 6 months. The 2016 Lancet Breastfeeding Series6 recorded the UK as having the lowest prevalence of breastfeeding in the world at 12 months of age (less than 1%). The infographic below illustrates the summary findings of the 2010 Infant Feeding Survey7 including some of the significant barriers to breastfeeding in the UK.
The introduction of the UNICEF UK Baby Friendly Initiative to hospitals in the UK in 199410 helped to improve breastfeeding initiation rates from low levels earlier in the 20th century. There is a high correlation between intention to breastfeed and initial feeding method. In 2010 98% of those intending to breastfeed went on to do so. Additionally, 18% of mothers who had planned in pregnancy to formula feed actually went on to breastfeed at the time of birth7.
There has previously been shown to be a substantial variation in breastfeeding rates in the four nations of the UK with initiation rates in 2010 highest in England at 83%, compared with 74% in Scotland, 71% in Wales, and 64% in Northern Ireland7. Exclusive breastfeeding at six weeks was 24% in England and 22% in Scotland, compared to 17% in Wales and 13% in Northern Ireland.
Many mothers are not informed that there is a significant increase in feeding at 5-6 weeks, as there is a change in milk at this stage which is stimulated by the babies increase in feeding.
In the Osteopathic practice we ensure all mums’ are informed about certain physiological changes that may cause them concern and think about stopping breastfeeding, especially when they feel they can’t cope. If they understand the first change is only for 2-4 days as the milk is established. The second change is at 5-6 weeks, when there is an increase in feeding to stimulate the milk change. If mums’ know it is only for 2-4 days and there is an end point, they can be supported through it. This is very important for their psychological wellbeing at a very fragile stage after birth.
The 2010 Infant Feeding Survey demonstrated that 83% of mothers reported that they knew about the health benefits of breastfeeding7 but knowledge of health benefits does not translate to high breastfeeding continuation rates. Common reasons for stopping breastfeeding include ‘insufficient milk’, the baby rejecting the breast or difficulty attaching at the breast (the ‘latch’) and pain.
Osteopathy has good reasons to support the function of how the baby can feed and what may be problematic e.g poor rotation of the neck in one direction, a difficult birth. This can affect the integration of the suck reflex through the cranial nerves that work together, including the nerve to the tongue. This is key to making sure the correct suck is there for good breastfeeding to be established. This can be compromised by tongue-tie, which may need to be dealt with by the midwife or surgeon and released surgically. This can give a quick and positive improvement in the suck, as the tongue can now squash the nipple up to the roof of the mouth and create a patent seal around the nipple; this creates suction and increases stimulation of the milk. The ‘tongue’(hypoglossal) nerve has been shown to have accessory connections to the vagus nerve which can be key in the aggravation of gut problems, as it connects with the sympathetic nervous system, which can lead to increased stimulation and pain within the stomach and gut. The most recent research shows that giving Lactobacillus reuteri to under 12 week old babies, is significant at improving colic, crying and regurgitation.
The survey showed that breastfeeding support is important to continuation in the early weeks. While 4 out of 5 women who experienced breastfeeding problems in the early days were offered help, those who did not receive help or support for problems were more likely to stop breastfeeding within the first 2 weeks7. The rate of continuation of breastfeeding decreases substantially within a few weeks, despite the fact that the majority of women would like to have breastfed for longer. Other factors like family and peer support from friends also impact on breastfeeding continuation, as does the need for mothers to return to work and the facilities made available in the workplace7.
Artificial Baby Milk Feeding in the UK
In the 2010 Infant Feeding Survey 31% of breastfed babies received supplements of formula, water or glucose in hospital, and this was more common for babies in special care, preterm babies and those receiving phototherapy. 73% had given their baby milk other than breastmilk by the age of six weeks, and 88% by six months7.
Infants who were given milk other than breastmilk by 8-10 months old were more likely to have been given ‘follow-on’ formula (57%) as their main breastmilk substitute, despite the fact that infant formula (also labelled ‘stage 1’ formula) is suitable for use up to the age of 1 year11.
Data showed that the preparation of powdered infant formula feeds according to three key safety recommendations had increased (49% up from 13% in 2005)7, 12,13. However, this does suggest that approximately half of the group receiving powdered infant formula were being fed formula prepared sub-optimally, with the associated risk of infection.
Introduction of Solid Foods in the UK
The timing of introduction of complementary solid foods was also studied in the 2010 Infant Feeding Survey. 30% of infants had been introduced to solids by 4 months, and 75% by 5 months7 . Whilst this was an improvement towards the recommended introduction of solids at 6 months compared with the 2005 survey, the figures still show a considerable variation from public health recommendations. Early introduction of solid food was more common amongst younger mothers and mothers from lower socioeconomic groups.
Following the decommissioning of the Infant Feeding Survey there is no subsequent national data collection on artificial milk feeding or the introduction of solid foods in the UK.
References
- The WI and the NCT: Support Overdue- Women’s Experiences of Maternity Services 2017
- Public Health England: Health Matters-Giving Every Child The Best Start in Life May 2016
- UK Department of Health: Infant Feeding Recommendation 2003
- NHS Website: Benefits of Breastfeeding
- WHO: Infant and Young Child Feeding Factsheet Updated February 2018
- Victora C, Bahl R, Barros A, França G, Horton S, Krasevec J et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475-490.
- Uk Infant Feeding Survey 2010
- NHS Digital: NHS Maternity Statistics (Initiation)
- Gov UK/Public Health England: Breastfeeding Statistics (6-8 weeks continuation data)
- Unicef UK Baby Friendly Initiative: About Baby Friendly
- NHS Website: Types of Formula Milk
- 1: make up only 1 feed at a time, 2: making feeds within 30 mins of water boiling, 3: adding water to the bottle before the powder (see ref 13 below)
- Food Standards Agency & Department of Health: Guidance for health professionals on safe preparation, storage and handling of powdered infant formula
Efficacy of probiotics for managing infantile colic due to their anti-inflammatory properties: a meta-analysis and systematic review
Reza Shirazinia 1, Ali Akbar Golabchifar 1, Mohammad Reza Fazeli 2
https://pubmed.ncbi.nlm.nih.gov/33848417/
Ong TG, Gordon M, Banks SS, Thomas MR, Akobeng AK.Cochrane Database Syst Rev. 2019 Mar 13;3(3):CD012473. doi: 10.1002/14651858.CD012473.pub2.PMID: 30865287 Free PMC article.
Anabrees J, Indrio F, Paes B, AlFaleh K.BMC Pediatr. 2013 Nov 15;13:186. doi: 10.1186/1471-2431-13-186.PMID: 24238101 Free PMC article. Review.
Karkhaneh M, Fraser L, Jou H, Vohra S.Paediatr Child Health. 2020 Apr;25(3):149-159. doi: 10.1093/pch/pxz007. Epub 2019 Apr 3.PMID: 32296276 Free PMC article. Review.
Published April 2017, Updated August 7th 2019